By Lisa Rowell
Every May, organizations like the American Stroke Association work to raise awareness about stroke risks, symptoms, and the urgency of seeking immediate medical help.
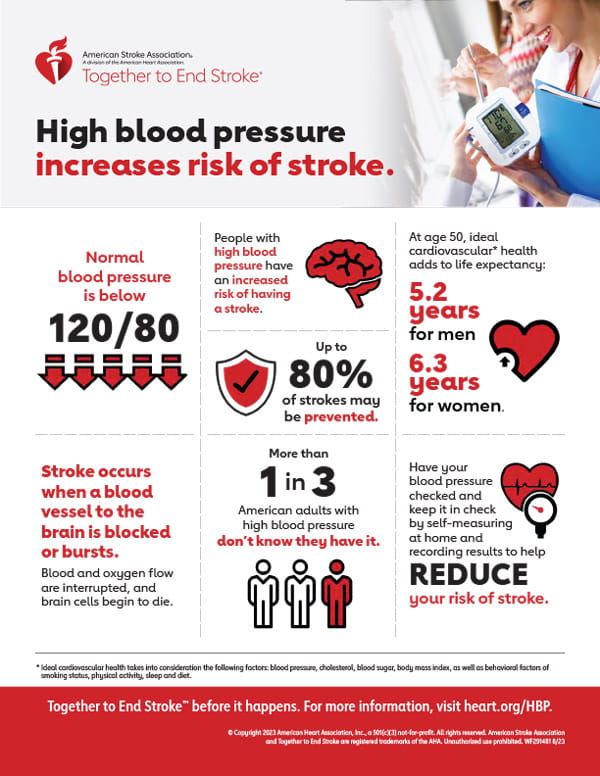
According to the American Heart Association’s 2025 Heart Disease and Stroke Statistics Update, stroke causes one in every 20 deaths in the U.S. The report highlights eight key health factors and behaviors that influence stroke and heart disease risk:
- Not smoking
- Regular physical activity
- Healthy diet
- Maintaining a healthy weight (71% of U.S. adults are overweight or obese)
- Proper sleep
- Controlling cholesterol (25.5% of U.S. adults have high LDL-C)
- Managing blood pressure
- Regulating blood sugar
While many of these are modifiable, uncontrollable risks include age, family history, previous stroke or heart attack, race, and gender. Other contributing factors may also play a role.
Stroke Statistics
The World Stroke Association reports over 795,000 strokes in the U.S. each year—about 610,000 of them first-time strokes.

Types of Stroke
Ischemic Stroke (87 percent of cases) is subacute and caused by a blocked blood vessel in the brain, often due to a clot. A cerebral embolism occurs when a clot forms elsewhere—usually the heart or major arteries—and travels to the brain. Atrial fibrillation (AF) is a common cause.
Hemorrhagic Stroke (13 percent of cases) is caused by bleeding in or around the brain, often from an aneurysm or arteriovenous malformation (AVM).
Other types include:
Transient Ischemic Attack (TIA) a temporary blockage that resolves within 24 hours but still requires emergency attention.
Cryptogenic Stroke has no identifiable cause.
Lacunar Stroke affects small, deep brain vessels.
Stroke Symptoms
Recognizing symptoms quickly can save lives. Use the FAST test:
- Face drooping
- Arm weakness
- Speech difficulty
- Time to call 911
Other signs include sudden numbness, weakness, or loss of speech or vision. Quick action is critical. Calling 911 ensures EMS can alert the hospital’s stroke team and begin care en route. Imaging like CT or MRI determines stroke type and guides treatment. Experts at Lake Cumberland Regional Hospital (LCRH) emphasize: do not drive—call 911.
Dr. Prostko’s story

Dr. Michael Prostko, is a hospitalist with Apogee Physicians at Lake Cumberland Regional Hospital. Many of the patients he cares for have suffered strokes. Now, as a stroke survivor himself, he shares his firsthand experience, offering insight into the importance of timely medical care and the recovery process.
October 3, 2024, did not begin like a typical morning for Dr. Prostko. He said he woke up and his foot didn’t quite feel right, but he went to work anyway.
“As I progressed through the morning, my arm started getting weaker and it became more and more difficult to walk,” he recalled.
Dr. Prostko went to the ER as a stroke alert around noon. “It was very rapid — a lot quicker that I thought it would be,” he said of the response.
“I was taken immediately to have a CT done,” which confirmed he had suffered a subacute stroke. Because of the nature of his stroke, he wasn’t eligible for Tenecteplase (TNK), a clot-busting agent.
Dr. Prostko said people often think a stroke happens in an instant. “It happened over the course of hours,” he said of the stroke he had.
He was admitted to the hospital’s Neuro Unit. By evening, he could no longer stand on his right leg. He underwent an MRI and frequent neurological exams. “I was getting weaker and weaker. I think I reached maximum weakness in the night – as best as I could figure.”
The medical staff monitored him for “drift,” where a stroke patient struggles to raise one arm. “Imagine holding two bowls of soup. You should be able to keep them level, but my right arm would have dropped the bowl,” he explained.
“It was very shocking and scary to me,” he said of the ordeal.
His condition also caused “foot drop,” where the toes remain on the ground while lifting the foot. He was quickly fitted with a brace, which he said helped significantly.
“I started working with therapy. I could only walk about 20-30 feet initially.”
While a patient at LCRH, Dr. Prostko said the stroke nurses took good care of him. “They are all very attentive. I needed help to get around and they immediately came and helped me,” he said.
Road to recovery
Stroke recovery varies by type and severity. The American Stroke Association says the fastest recovery usually happens in the first three to four months.
Within days, Dr. Prostko was using a walker and transferred to the Rehab Unit for two weeks.
“I was getting three hours of rehab a day and an hour and a half of occupational therapy,” he said.
“Dewayne was my main occupational therapist and he was just fantastic.”
“I had several physical therapists and they were all very good. I progressed from really not walking at all to walking about 150 feet.”
After discharge, he continued occupational therapy at home.
Continual hard work
“It’s been continual gains since then,” he said. “Twenty-four hours after the initial stroke I could barely walk or stand. Now I am independent — but that was a long road.”
He walked tracks, the mall—anywhere he could—pushing through fatigue.
“Now I can do it all without even a cane but it still fatigues me,” he said.
He returned to work in December.
“It was definitely a lot harder than I expected,” he admitted. By January, he was back full-time.
Challenges remain
“My hand and forearm are numb, and my shoulder is numb. I can’t lay on my right side.”
“I have a lot of hand numbness and weakness,” he said. “I can’t really throw a ball or anything with my right arm… Typing is slow but I can use my right hand a little bit for typing.”
A physician’s perspective
“What I had was a typical stroke,” Dr. Prostko said. “It’s an ischemic stroke where it killed off some nerve cells.” He said most patients with this type of stroke an be treated effectively at LCRH without transfer. He emphasized early rehab: “I spent two weeks using a walker, and then I was walking with a cane.”
Recovery is physical and emotional. “It’s a lot of work. It can get people depressed,” he said. “You’re not able to do things and you get depressed.” While he didn’t struggle with depression, he said it’s critical to address.
“I know if you work really hard you can definitely make gains. My advice to those who’ve had a stroke is: do your therapy — and then do your therapy at home.”
He credits progress to persistence. “You get exhausted but you don’t want to get too exhausted. It’s just really effort, effort, effort… If I took a break I went backwards. It’s a forward hard situation.”
He praised both the inpatient and outpatient therapy teams.
“They challenge you to find where your deficits are.”
“I haven’t hit my ‘new normal’ yet. I will always have deficits. I’ve gotten a lot back and it’s through working at it.”
Final thoughts
Seeing stroke from both sides—physician and survivor—gave Dr. Prostko new perspective. “It’s a new understanding of their situation,” he said.
He commended LCRH’s stroke response, noting they may see 10-12 cases a week, or even three in a day. Some are short TIAs — often warning signs of more serious events.
He urged people to watch their habits — especially smoking, fried foods, and unmanaged blood pressure.
Dr. Prostko’s journey is a testament to early care, persistent rehab, and the dedication of the stroke team.
Resources include the World Stroke Organization: world-stroke.org/en/; the American Stroke Association: stroke.org/en/; Centers for Disease Control and Prevention: cdc.gov/stroke/index.html

